
Kidney disease
While chronic kidney disease is often detected too late to be reversible, it can be prevented by a healthy lifestyle, or treated if detected early.
Between July 2017 and June 2019, care involving dialysis was the leading cause of hospitalisation among First Nations people, accounting for 44% (474,745) of all hospitalisations. Excluding dialysis, there were 6,710 hospitalisations for First Nations people due to chronic kidney disease.
Patients with kidney failure, also known as end-stage kidney disease, require either a kidney transplant or dialysis to maintain the functions normally performed by the kidneys. These treatments are collectively known as ‘kidney replacement therapy’.
In the 3-year period 2019–2021, 1,063 First Nations people began kidney replacement therapy for kidney failure. This corresponds to an incidence rate of 41 new cases of kidney failure with replacement therapy for every 100,000 First Nations people.
In 2019–2021, among First Nations people who began receiving kidney replacement therapy, the most common type of primary kidney disease was diabetic kidney disease (also known as diabetic nephropathy) – experienced by 71% (753) of the 1,063 new First Nations kidney replacement therapy patients. This was followed by glomerulonephritis (77 or 7.2%) and hypertension (61 or 5.7%).
The incidence of kidney failure with replacement therapy was 6 times as high for First Nations people as for non-Indigenous Australians (63 compared with 10 per 100,000 population, based on age-standardised rates). Between 2012 and 2021, the age-standardised incidence rate for kidney failure with replacement therapy did not change significantly for First Nations people. For non-Indigenous Australians, there was a 7.8% increase in the age-standardised incidence rate for kidney failure with replacement therapy, which was mainly driven by increases among non-Indigenous males (10% increase over the period) (Figure 4.22).
Figure 4.22: Incidence of kidney failure with replacement therapy among First Nations people by remoteness (crude rates, 2019–2021), and by Indigenous status over time (age-standardised rates, 2012 to 2021)

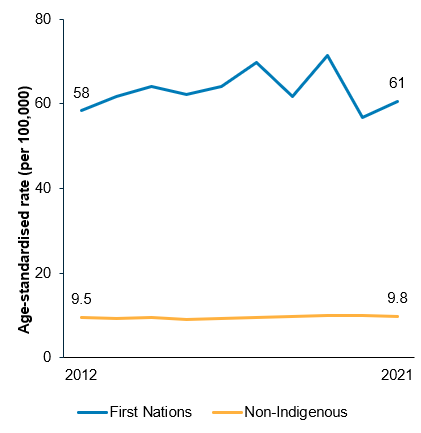
Source: Measure 1.10, Table D1.10.13 and Table D1.10.12 – AIHW analysis of Australia and New Zealand Dialysis and Transplant Registry data.
As at 31 December 2021, there were 2,568 First Nations people with kidney failure who were receiving kidney replacement therapy, a prevalence rate of 289 per 100,000 population. Most First Nations patients with kidney failure (85% or 2,170 patients) were receiving dialysis, while 15% (or 398 patients) had received a kidney transplant. In comparison, about one-half (49%; 12,063 of 24,774 patients) of non-Indigenous patients received a kidney transplant.
In the 6-year period 2016–2021, 1,381 First Nations people were reliant on dialysis to manage their kidney failure at the time of their death, based on underlying cause of death. The primary cause of death in over one-third (466 deaths or 34%) of these cases was cardiovascular diseases, a further one-fifth (307 deaths or 22%) was due to withdrawal from dialysis and 12% (161 deaths) was due to infections. Among First Nations people who had received a transplant to manage their kidney failure, there were 49 deaths in 2016–2021 – the leading cause of these deaths was cardiovascular disease (13 deaths or 27%), followed by cancer (7 deaths or 14%), infections, and withdrawal (both 6 deaths or 12%).
Kidney diseases were the 10th leading cause of death for First Nations people (1.8% of deaths). First Nations females accounted for 58% of deaths due to kidney disease among First Nations people.
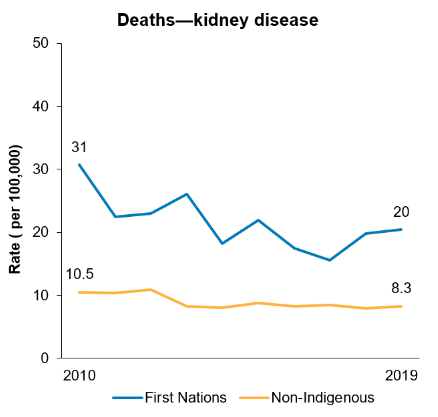
Between 2010 and 2019, the age-standardised death rate from kidney disease among First Nations people decreased by 36%. However, there was no significant reduction in the gap between First Nations people and non-Indigenous Australians over this period (data from New South Wales, Queensland, Western Australia, South Australia, and the Northern Territory combined) (Figure 4.23).
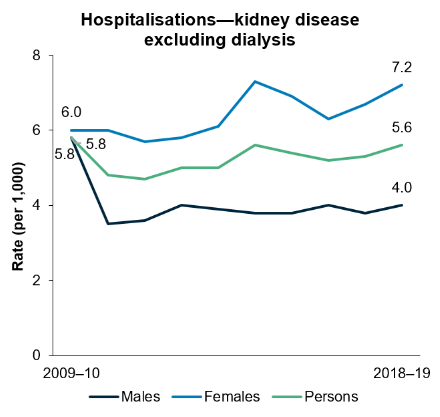
Over the decade from 2009–10 to 2018–19, the age-standardised hospitalisation rate for a principal diagnosis of chronic kidney disease increased by 6% for First Nations people. This trend was driven by the increases for First Nations females (by 22%) as the rate among First Nations males declined (by 16%) (Figure 4.23).
Figure 4.23: Rates of hospitalisations due to kidney disease (2009–10 to 2018–19) among First Nations people, and deaths due to kidney disease by Indigenous status and sex (2010–2019) (age-standardised)
Notes
1. Data on hospitalisations from New South Wales, Victoria, Queensland, Western Australia, South Australia, and the Northern Territory combined.
2. Data on deaths from New South Wales, Queensland, Western Australia, South Australia, and the Northern Territory combined.
Source: Measure 1.10, Table D1.10.20 – AIHW analysis of National Hospital Morbidity Database; and Measure 1.10, Table D1.23.23 – AIHW National Mortality Database.
Kidney disease is more likely to be recorded as an additional diagnosis on hospitalisation administrative records or recorded on death certificates as an associated cause compared with other diseases. The above estimations of the impact of kidney disease are based on the principal diagnosis of hospitalisation or underlying cause of death, and therefore likely underestimate the true extent of chronic kidney disease among First Nations people.
For further information, see: