
5. Tier 2 – Determinants of health
Health is influenced by social determinants and individual health risk factors. Social determinants of health refer to the circumstances in which people are born, grow up, live, work and age, and the systems put in place to deal with illness. These circumstances are in turn shaped by a wider set of forces such as economics, social policies, and politics (Commission on Social Determinants of Health 2008).
Using a composite measure based on a number of survey questions about self-assessed health, long-term health conditions, and emotional wellbeing, AIHW analysis of ABS surveys for 2017–18 and 2018–19 estimated that around 3 in 10 (29%) First Nations people aged 18–64 had ‘good health’.
After accounting for the differences in average age, sex, marital status, remoteness, and state and territory between First Nations and non-Indigenous survey respondents, the health gap between First Nations people and non-Indigenous Australians was 24 percentage points – a decrease from 27 percentage points in 2011–13.
Almost two-thirds (65%) of the heath gap was explained by a set of 11 selected factors that were broadly classified into 2 groups: social determinants of health (35%, 5 factors) and health risk factors (30%, 6 factors). An estimated 20% of the explained health gap was attributed to the overlap, or interactions, between the social determinants and health risk factors (Figure 5.1).
Of the 35% of health gap due to social determinants, the largest effects were due to differences in employment status and hours worked (contributing to 14% of the health gap), equivalised household income (13% of the health gap), and the highest level of school attainment (8.9% of the health gap).
Of the 30% of the health gap due to risk factors, the largest effects were due to differences in current smoking rates (contributing 13% of the health gap) and overweight and obesity rates (11% of the health gap).
This analysis did not explain about 35% of the health gap. The unexplained health gap includes possible effects from factors that might have contributed to good health but were not available in the survey data analysed. For example, these factors could include access to affordable and culturally appropriate health care services, connection to country and language, and effects of structural disadvantage and racism.
Figure 5.1: Proportion of the adjusted health gap explained by differences in social determinants and health risk factors between First Nations people and non-Indigenous Australians aged 18–64, 2017–19
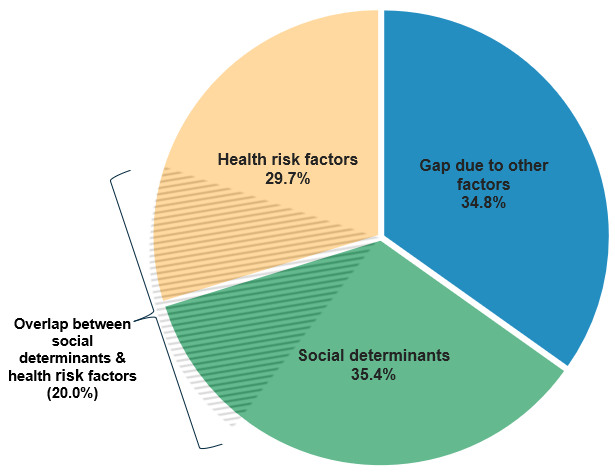
Note: Gap due to other factors refers to the component of the gap unexplained by differences in the factors included in this study. This reflects the fact that the available data do not provide a complete picture of the differences between the two populations.
Source: AIHW analysis of ABS NATSIHS 2018–19 and ABS NHS 2017–18, as published in Australia’s Health 2024: data insights (AIHW 2024b).
Together, household income (adjusted for household size and composition), employment status or number of hours worked, and smoking status account for 40% of the total health gap.
If First Nations adults were to have the same average equivalised household income, same average employment rate and hours worked, and same average smoking rate levels as non-Indigenous adults, the health gap would be reduced by more than a third – from 24 percentage points to around 14 percentage points.
In comparison with the previous analysis of data from 2011–13 (AIHW 2018):
- The overall size of the adjusted health gap has decreased by 2.9 percentage points (from 27 to 24 percentage points).
- The unexplained component of the adjusted health gap has decreased by 12 percentage points from 47% to 35%, largely due to a substantial increase of 11 percentage points in the proportion of the health gap explained by health risk factors, which rose from 19% to 30%.
- The proportion explained by social determinants has increased, by 1 percentage point from 34% to 35%.
- Among the health risk factors, the largest changes were in the proportions of the health gap explained by Body Mass Index (BMI) and smoking status. The proportion of the health gap explained by BMI has increased by 3.6 percentage points from 7.2% to 11%, and the proportion explained by smoking has increased by 3.3 percentage points from 10% to 13%.
Figure 5.2: Contribution of individual social determinants and health risk factors to the adjusted health gap between First Nations people and non-Indigenous Australians aged 18–64, 2017–19
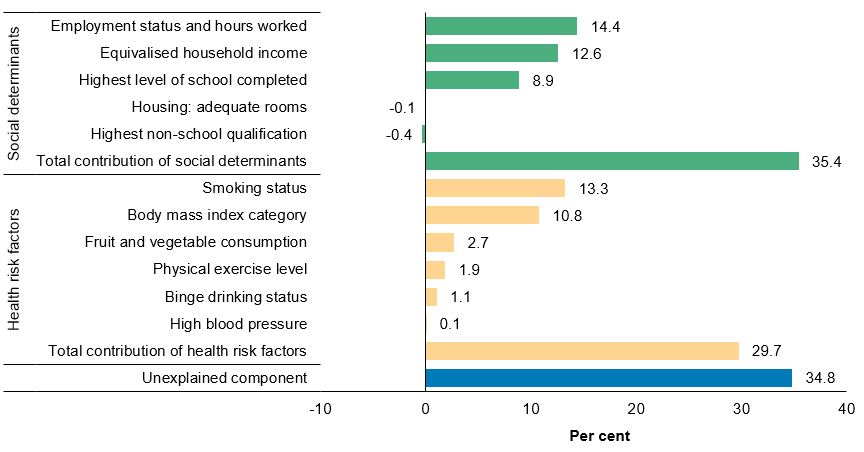
Note: For additional analyses, see Australia’s health 2024: data insights (AIHW 2024b).
Source: AIHW analysis of ABS NATSIHS 2018–19 and ABS NHS 2017–18, published in Australia’s Health 2024: data insights (AIHW 2024b).