
Mental health and social and emotional wellbeing
The broad disease group that is the leading cause of disease burden for Aboriginal and Torres Strait Islander (First Nations) people is mental and substance use disorders, which includes depressive disorders, bipolar disorder, anxiety disorders, schizophrenia and alcohol and drug use disorders.
Most of the disease burden from mental and substance use disorders is non-fatal – that is, it is due to years spent living with illness.
Maintaining high levels of social and emotional wellbeing is now a focus of the National Agreement, as reflected in Target 14: Significant and sustained reduction in suicide of Aboriginal and Torres Strait Islander people towards zero – see the Closing the Gap Information Repository.
The National Aboriginal and Torres Strait Islander Health Plan 2021-2031, released in December 2021, provides a strong overarching policy framework to ensure the formal partnership and shared decision making between the Australian Government and First Nations communities. The Health Plan covers a range of health services including mental health, and social and emotional wellbeing.
The National Strategic Framework for Aboriginal and Torres Strait Islander Peoples’ Mental Health and Social and Emotional Wellbeing (Commonwealth of Australia 2017) and the National Mental Health and Suicide Prevention Plan (Department of Health and Aged Care 2021a) are important components of the national response to the health of First Nations people.
While intentional self-harm and suicidal behaviour are classified as injuries for burden of disease analysis, in the HPF they are reported under measure 1.18 Social and emotional wellbeing. Some information on intentional self-harm and deaths by suicide is presented in this section and in the following section on injury.
Almost 1 in 3 First Nations adults (31%) had high to very high levels of psychological distress in 2018–19 (age-standardised), a similar proportion to 2014–15. In comparison, 13% of non-Indigenous adults had high levels of psychological distress. Those who had been removed from families or had relatives removed from families had a higher proportion with high or very high levels of psychological distress (38%) compared to those who did not have these experiences (26%).
In 2014–15, 68% of First Nations people aged 15 and above (303,300) reported that in the previous year they had experienced one or more specified personal stressors – that is, events with the potential to adversely affect their health or wellbeing, such as serious illness or the death of a family member or friend (see Table 4.2 for most common personal stressors).
Table 4.2: Most common personal stressors, First Nations people aged 15 and over, by remoteness, 2014–15
|
Sources of stress |
Non-remote Number |
Non-remote Per cent |
Remote Number |
Remote Per cent |
|---|---|---|---|---|
|
Death of a family member or close friend |
89,100 |
26% |
33,400 |
35% |
|
Not able to get a job |
63,500 |
18% |
18,200 |
19% |
|
Serious illness |
45,100 |
13% |
8,600 |
8.9% |
|
Mental illness |
40,200 |
12% |
5,500 |
5.7% |
|
Overcrowding at home |
20,100 |
5.8% |
9,000 |
9.3% |
|
Alcohol-related problems |
20,500 |
5.9% |
8,600 |
8.9% |
Note: Proportion of all First Nations people aged 15 and over, more than one response could be given.
Source: Measure 1.18, Table D1.18.4 – AIHW and ABS analysis of National Aboriginal and Torres Strait Islander Social Survey 2014–15.
Intentional self-harm and suicide
Between July 2017 and June 2019, 5,829 First Nations people were hospitalised due to intentional self-harm (0.9% of all hospitalisations of First Nations people, excluding dialysis). This corresponds to a rate of 3.5 hospitalisations per 1,000 population for First Nations people.
Among First Nations people, rates of hospitalisations for intentional self-harm were higher among females than males (4.4 compared with 2.6 hospitalisations per 1,000, based on crude rates). For First Nations males, the hospitalisation rate for intentional self-harm was highest for those aged 35–44 (5.2 hospitalisations per 1,000 population). For First Nations females, the rate for was highest for those aged 15–24 (9.2 hospitalisations per 1,000 population) (Figure 4.9).
First Nations people were hospitalised for intentional self-harm at nearly 3 times the rate of non-Indigenous Australians, based on age-standardised rates. The largest relative differences in rates between First Nations people and non-Indigenous Australians (4.5 times) was in the 35–44 age group, with rates being 4.3 times as high for males and 4.6 times as high for females.
Figure 4.9: Rate of hospitalisations due to intentional self-harm, by Indigenous status, age group and sex, July 2017 to June 2019

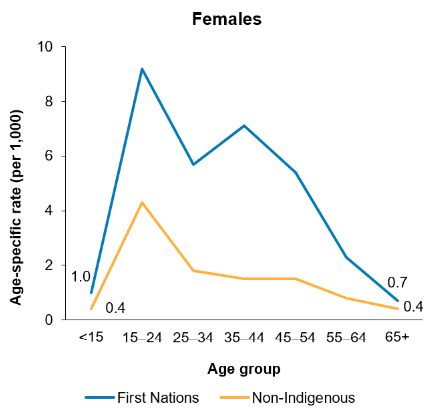
Source: Measure 1.18, Table D1.18.27 – AIHW analysis of National Hospital Morbidity Database.
In 2015–2019, 847 First Nations people died from intentional self-harm (suicide), a rate of 24 suicide deaths per 100,000 population. Suicide accounted for approximately 5.5% of total deaths among First Nations people. The age-standardised suicide rate for First Nations people increased by 30% over the decade from 2010 to 2019 based on linear regression analysis, with the rate also increasing for non-Indigenous Australians (by 24%) (data from New South Wales, Queensland, Western Australia, South Australia, and the Northern Territory combined) (Figure 4.10). This corresponded to a significant widening (by 38%) of the gap between First Nations people and non-Indigenous Australians.
Figure 4.10: Suicide rates, by Indigenous status (age-standardised), 2010–2019
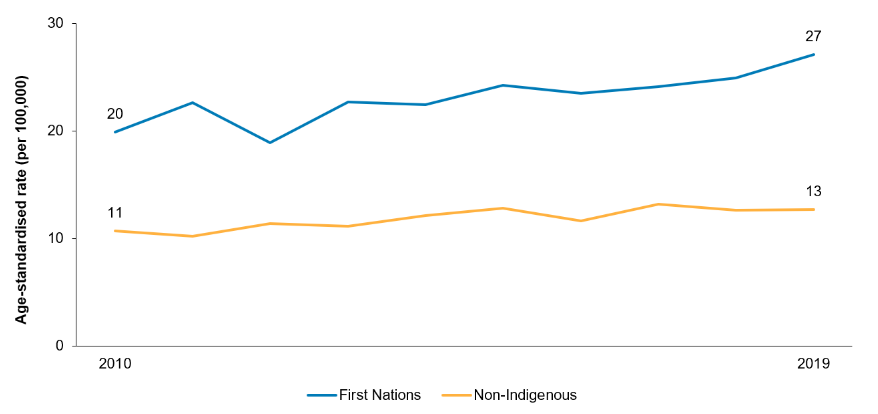
Note: Data New South Wales, Queensland, Western Australia, South Australia, and the Northern Territory combined.
Source: Measure 1.18, Table D1.18.26 – AIHW National Mortality Database.
The death rate due to suicide was highest for First Nations males aged 30–34 (77.8 per 100,000) and for First Nations females aged 15–19 (27.5 deaths per 100,000 population) in 2015–2019 (data from New South Wales, Queensland, Western Australia, South Australia, and the Northern Territory combined). Among non-Indigenous Australians, the suicide death rate was highest for males aged 45–49 (30.5 deaths per 100,000 population) and females aged 45–49 and 50–54 (both 9.7 deaths per 100,000 population) (Figure 4.11). The overall rate of deaths from suicide for First Nations people was 2 times the rate of non-Indigenous Australians.
Figure 4.11: Suicide rates, by Indigenous status, age group and sex, 2015–2019
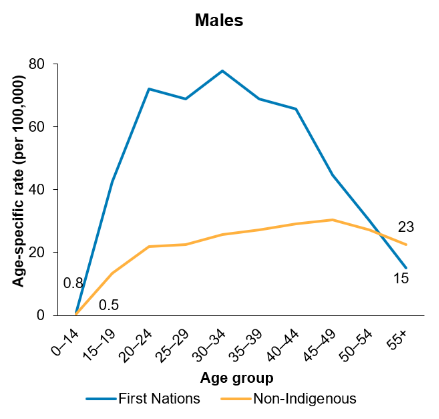
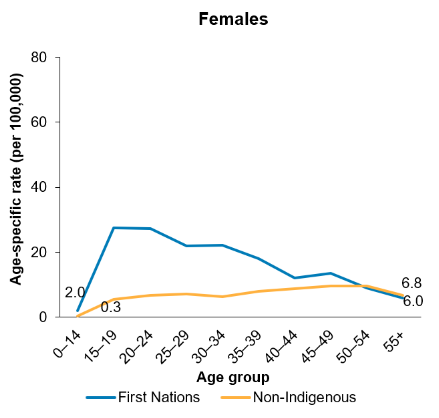
Note: Data from New South Wales, Queensland, Western Australia, South Australia, and the Northern Territory combined.
Source: Measure 1.18, Table D1.18.22 – AIHW and ABS National Mortality Database.
For further information, see: