
Key messages
- In 2018–19, 3 in 10 Aboriginal and Torres Strait Islander people aged 15 years and over reported that they had abstained from alcohol in the previous 12 months.
- 50% of Indigenous Australians aged 15 years and over partook in single occasion risky alcohol consumption (more than four standard drinks) in 2018–19, down from 54% in 2012–13.
- In 2018–19, 18% of Indigenous Australians aged 15 years and over reported exceeding the lifetime alcohol risk guidelines (more than two standard drinks per day on average).
- Indigenous males were hospitalised due to alcohol at 1.4 times the rate of Indigenous females (810 per 100,000 compared with 584 per 100,000) from July 2017 to June 2019.
- Alcohol-related hospitalisation rates increased by 36% for Indigenous females (from 539 to 724 per 100,000) and by 11% for Indigenous males (from 928 to 1,125 per 100,000) from 2009–10 and 2018–19 (age-standardised).
- In 2015–2019, there were 458 alcohol-related deaths of Indigenous Australians – of these, 63% were due to alcoholic liver disease (288 deaths).
- Since the implementation of a community led program in 2010 to lower the risk of Fetal Alcohol Spectrum Disorders (FASD) in the Fitzroy Valley, Western Australia, alcohol use during pregnancy declined from 61% in 2010 to 31.9% in 2015. The project highlights the impact of community-led strategies, such as educating the community on the harms of alcohol consumption during pregnancy, on reducing and eliminating FASD.
- Research has shown that the proportion of admission to the Alice Springs Hospital intensive care units for acute alcohol misuse in the Northern Territory dropped by 54% in the first six months after the introduction of the minimum unit price (MUP) on alcohol in October 2018.
Why is it important?
Alcohol consumption is a complex, multi-determined behaviour, influenced by a range of biological and environmental factors, social and economic determinants and emotional wellbeing factors, including trauma, coping with stress, and peer pressure (House of Representatives Standing Committee on Indigenous Affairs 2015).
Excessive consumption of alcohol is associated with health and social problems in all populations (NHMRC 2008). The 2020 Australian Guidelines to Reduce Health Risks from Drinking Alcohol provide the current advice from the National Health and Medical Research Council (NHMRC) around alcohol consumption (NHMRC 2020). These guidelines have informed the survey data compiled for this measure.
Long-term excessive alcohol consumption is associated with a variety of adverse health and social consequences. It is a major risk factor for health conditions, including liver disease, pancreatitis, heart disease, stroke, diabetes, obesity and some types of cancer. It is also linked to social and emotional wellbeing, mental health and other drug issues (NHMRC 2020). When mothers have consumed alcohol during pregnancy, babies may be born with Fetal Alcohol Spectrum Disorders (FASD) (Telethon Institute for Child Health Research 2009).
Single occasion risky alcohol consumption can have negative health effects such as acute intoxication, and may influence people to engage in harmful behaviours that increase the risk of injury, transport accidents, self-harm, and risky sexual activity (NHMRC 2020).
Harmful alcohol consumption can also affect families and communities. It has the potential to lead to anti-social behaviour, violence, assault, imprisonment and family breakdown (NHMRC 2020).
Aboriginal and Torres Strait Islander people are more likely to abstain from alcohol than non-Indigenous Australians; however those who do drink are more likely to do so at dangerous levels.
The National Aboriginal and Torres Strait Islander Health Plan 2021-2031 (the Health Plan), released in December 2021, provides a strong overarching policy framework for Aboriginal and Torres Strait Islander health and wellbeing and is the first national health document to address the health targets and priority reforms of the National Agreement on Closing the Gap.
‘Focusing on prevention’, including health promotion, is one of the key priority areas of the Health Plan, and one objective specifically addresses alcohol consumption:
- Objective 4.6 Deliver targeted, needs-based and community-driven actions to prevent alcohol and other drug related harm
The Health Plan is discussed further in the Implications section of this measure.
Burden of disease
In 2018, alcohol use disorders accounted for 4.4% of total disease burden among Indigenous Australians (10,568 disability adjusted life years (DALYs)). For Indigenous males aged 25–44 years, alcohol use disorders were the leading contributor to total burden (12% or 4,656 DALYs) (followed by suicide and self-inflicted injuries, and anxiety disorders).
Considering alcohol use as a risk factor for disease and injury, it was estimated that 10.5% of total disease burden among Indigenous Australians was due to alcohol use. Alcohol use was the leading risk factor contributing to disease burden for Indigenous males aged 15–24 years and accounted for 26% of total disease burden in males in this age group (4,283 DALYs). Among Indigenous males aged 25–44 years, alcohol use was the leading risk factor and accounted for just under one-quarter (23% or 9,045 DALYs) of total disease burden among this group (AIHW 2022).
Data findings
In 2020, the NHMRC published updated alcohol guidelines, advising consumption of no more than ten standard drinks a week reduces the lifetime risk of harm from alcohol-related disease or injury; and drinking no more than four standard drinks on a single occasion reduces the risk of alcohol-related injury arising from that occasion (NHMRC 2020).
This measure presents data on single occasion risk and lifetime risk from the 2018–19 National Aboriginal and Torres Strait Islander Health Survey, which were defined according to the NHMRC’s previously released 2009 guidelines that applied at the time the survey was undertaken. These guidelines were: no more than 4 standard drinks on a single occasion reduces the risk of alcohol related injury arising from that occasion (single occasion risk) and no more than two standard drinks on any day reduces the lifetime risk of harm from alcohol-related disease or injury (lifetime risk).
Abstinence
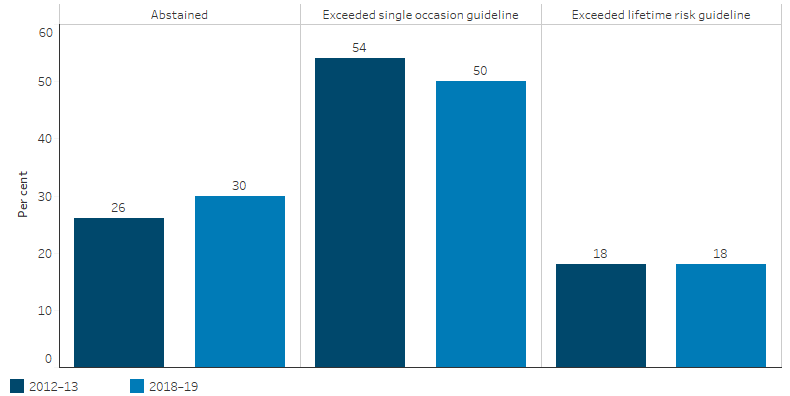
The 2018–19 National Aboriginal and Torres Strait Islander Health Survey included questions about alcohol consumption, including the amount consumed on single occasions and frequency of drinking. In 2018–19, 30% of Indigenous Australians aged 15 years and over reported that they had abstained from alcohol in the previous 12 months or never consumed alcohol (Table D2.16.18). In 2012–13, the proportion was 26% (ABS 2013) (Figure 2.16.1).
Figure 2.16.1: Alcohol risk levels, Indigenous Australians aged 15 and over, 2012–13 and 2018–19
Source: Table D2.16.21. AIHW and ABS analysis of National Aboriginal and Torres Strait Islander Health Survey, 2018–19; Australian Aboriginal and Torres Strait Islander Health Survey 2012–13 (ABS Table 14_3).
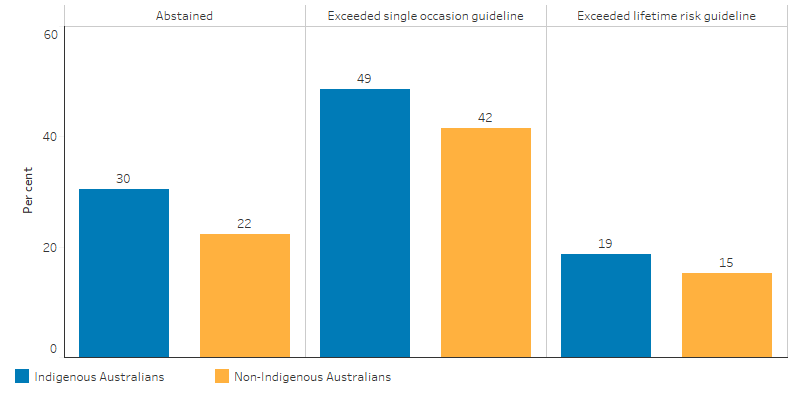
After adjusting for differences in the age structure between the two populations, Indigenous Australians aged 15 years and over were 1.4 times as likely to have abstained from drinking alcohol in the previous 12 months as non-Indigenous Australians (30% and 22%, respectively) in 2018–19 (ABS 2019) (Figure 2.16.2).
Single occasion risky alcohol consumption
In 2018–19, 50% of Indigenous Australians aged 15 years and over exceeded the single occasion risk guidelines at least once in the 2 weeks prior to the survey (Table D2.16.19). This was down from 54% in 2012–13 (ABS 2013) (Figure 2.16.1).
The incidence of exceeding the single occasion risk guidelines was higher for Indigenous males (61%) than Indigenous females (40%) and was similar in non-remote areas (Major cities, Inner and Outer regional areas combined) (50%) and remote areas (Remote and Very remote areas combined) (49%) (Table D2.16.19).
Of Indigenous Australians aged 15 years and over who exceeded the single occasion risk guidelines, 18% drank at least once a week and 32% drank less than once a week (Table D2.16.9).
After adjusting for differences in the age structure between the two populations, Indigenous Australians aged 15 years and over exceeded the single occasion alcohol risk guidelines at 1.2 times the rate of non-Indigenous Australians (49% and 42%, respectively) (ABS 2019) (Figure 2.16.2).
Figure 2.16.2: Age-standardised alcohol risk levels for persons aged 15 and over, by Indigenous status, 2018–19
Source: AIHW and ABS analysis of National Aboriginal and Torres Strait Islander Health Survey 2018–19 (ABS Table 13.3).
In 2018–19, Indigenous Australians aged 18–24 years were most likely to exceed the single occasion alcohol risk guidelines (65%) and those aged 15–17 years had the lowest rate (18%) (Table D2.16.19).
Lifetime risk
In 2018–19, 18% of Indigenous Australians aged 15 years and over drank at levels that exceeded the NHMRC lifetime risk guidelines (Table D2.16.20). This was the same in 2012–13 (ABS 2013) (Figure 2.16.1).
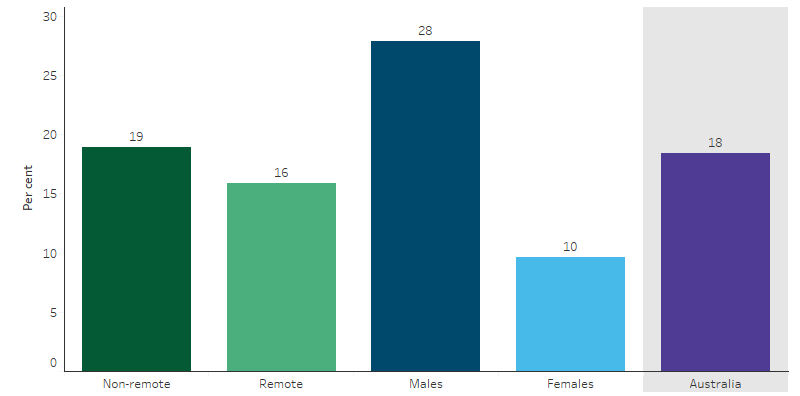
The rate of exceeding the lifetime alcohol risk guidelines was higher for Indigenous males than Indigenous females (28% and 10%) and higher in non-remote areas than remote areas (19% and 16%) (Table D2.16.20, Figure 2.16.3).
After adjusting for differences in the age structure between the two populations, Indigenous Australians aged 15 years and over exceeded the lifetime alcohol risk guidelines at 1.2 times the rate of non-Indigenous Australians (19% and 15%, respectively) (ABS 2019) (Figure 2.16.2).
Of Indigenous Australians who exceeded the lifetime risk guidelines in 2018–19, 37% consumed two to three standard drinks daily, 15% consumed three to four standard drinks, and 48% consumed more than four standard drinks. For non-Indigenous Australians who exceeded the lifetime risk guidelines, 39% consumed two to three standard drinks, 23% consumed three to four and 38% consumed more than four standard drinks (ABS 2019).
Figure 2.16.3: Indigenous Australians aged 15 and over who exceeded the lifetime alcohol risk guidelines, by remoteness and sex, 2018–19
Source: Table D2.16.20. AIHW and ABS analysis of National Aboriginal and Torres Strait Islander Health Survey 2018–19.
Limitations of survey data
The survey data indicate the prevalence of alcohol consumption but underestimate actual consumption. Further, it cannot be assumed that patterns of consumption are uniform across geographic regions (Stockwell et al. 2004). After considering a range of evidence, a review by Wilson and others estimated the prevalence of harmful alcohol use in the Indigenous population at twice that of the non-Indigenous population (Wilson et al. 2010).
Effect on communities
Excess alcohol consumption affects communities. In 2014–15, 19% of Indigenous Australians aged 15 years and over reported experiencing a family stressor related to alcohol problems. The rate was higher in remote areas (23%) than non-remote areas (18%).
One study in New South Wales found that, after controlling for social and demographic variables, the rate of offensive behaviour and property damage tended to be higher in areas with higher levels of alcohol sales (Stevenson et al. 1999). There is also a clear link between alcohol and violence and imprisonment (see measure 2.11 Contact with the criminal justice system).
Hospitalisation
Over the period July 2017 to June 2019, there were 11,576 hospitalisations of Indigenous Australians with a principal diagnosis related to alcohol use, which represented 1.9% of all hospitalisations of Indigenous Australians (excluding dialysis) and corresponded to a rate of 697 hospitalisations per 100,000 population (Table D2.16.11, Table D1.02.1).
The rate of hospitalisations related to alcohol use for Indigenous males was 1.4 times the rate of Indigenous females (810 per 100,000 compared with 584 per 100,000).
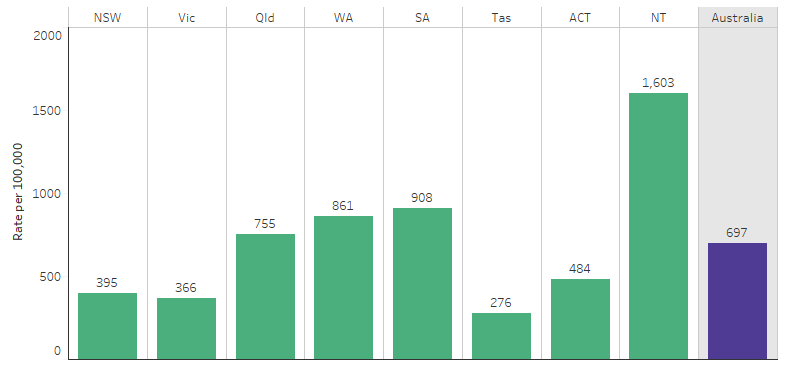
Hospitalisation rates related to alcohol use for Indigenous Australians were highest in Remote areas (1,472 per 100,000), followed by Very remote areas (1,146 per 100,000), with the lowest rate in Inner regional areas (305 per 100,000) (Table D2.16.12). By jurisdiction, hospitalisations related to alcohol use for Indigenous Australians were highest in the Northern Territory (1,603 per 100,000) and lowest in Tasmania (276 per 100,000) (Table D2.16.15, Figure 2.16.4).
Figure 2.16.4: Rate of hospitalisations among Indigenous Australians that were related to alcohol use, by jurisdiction, July 2017 to June 2019
Source: Table D2.16.15. AIHW analysis of National Hospital Morbidity Database.
By age group, the rate of alcohol-related hospitalisations was lowest for Indigenous Australians aged 0–14 (18 per 100,000) and increased in each subsequent 10-year age group through to 45–54 (2,221 per 100,000) before decreasing to 456 per 100,000 for those aged 65 years and over (Table D2.16.14).
Acute intoxication was the most common cause of alcohol-related hospitalisations for Indigenous (60% of the 11,576 alcohol-related hospitalisations), followed by dependence syndrome (14%), withdrawal (10%) and alcoholic liver disease (7.5%), harmful use of alcohol (2.9%) and psychotic disorders associated with alcohol use (1.9%). For non-Indigenous Australians, the most common causes were dependence syndrome (52%), acute intoxication (19%), withdrawal (9.4%) and alcoholic liver disease (7.5%) (Table D2.16.11).
After adjusting for differences in the age structure between the two populations, Indigenous Australians were hospitalised with alcohol-related diagnoses at 3.6 times the rate of non-Indigenous Australians. The difference between the two populations was largest for those 45–54, with Indigenous Australians in this age group hospitalised at 4.4 times the rate of non-Indigenous Australians (Table D2.16.14).
Looking at specific types of alcohol-related hospitalisations, age-standardised hospitalisation rates were: 14 times as high for Indigenous Australians as for non-Indigenous Australians for psychotic disorders; 11 times as high for acute intoxication; 4.1 times as high for alcoholic liver disease; and 3.9 times as high for withdrawal (Table D2.16.11).
Deaths
Deaths data in this measure are from five jurisdictions for which the quality of Indigenous identification in the deaths data is considered to be adequate; namely, New South Wales, Queensland, Western Australia, South Australia, and the Northern Territory (see Data sources: National Mortality Database).
Among Indigenous Australians in the 5-year period 2015–2019, there were 458 alcohol-related deaths, at a rate of 13 per 100,000 population. Indigenous males accounted for just over two-thirds (313 deaths or 68%) of these deaths, a lower proportion than that of non-Indigenous males (75%). Indigenous males died due to alcohol use at 2.1 times the rate of Indigenous females (17 compared with 8.1 deaths per 100,000, respectively).
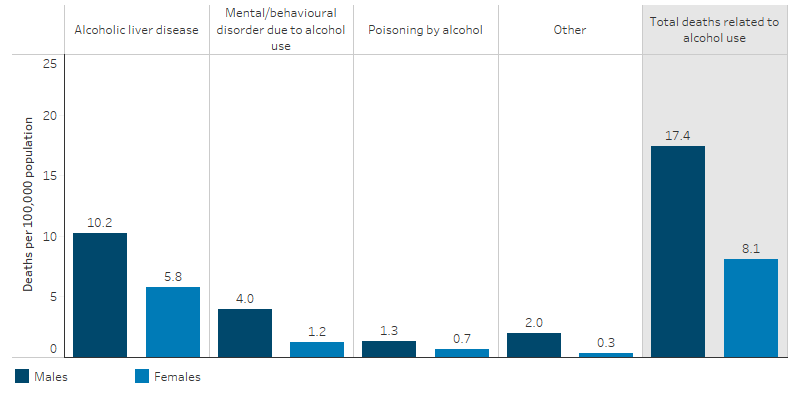
Among Indigenous Australians the leading cause of alcohol-related deaths were due to alcoholic liver disease, which accounted for almost two-thirds (288 deaths or 63%) of the deaths. This was followed by mental and behavioural disorders due to alcohol use (92 deaths or 20%) (for example, depressive disorders secondary to alcohol consumption). For Indigenous males, the rate of death due to alcoholic liver disease was 1.8 times the rate of Indigenous females (10.2 and 5.8 per 100,000, respectively) and for mental and behavioural disorders due to alcohol use the rate was 3.3 times that of Indigenous females (4.0 and 1.2 per 100,000, respectively) (Figure 2.16.5).
Figure 2.16.5: Rate of death related to alcohol use, Indigenous Australians, by sex, NSW, Qld, WA, SA and the NT, 2015–2019
Source: Table D2.16.10. AIHW National Mortality Database.
After adjusting for differences in the age structure between the two populations, Indigenous Australians were 4.2 times as likely to die from alcohol-related deaths as non-Indigenous Australians. Indigenous Australians were 3.8 times as likely to die from alcoholic liver disease as non-Indigenous Australians and 4.7 times as likely to die from mental and behavioural disorders due to alcohol use (Table D2.16.10).
Alcohol-related death was responsible for 4.1% of the total gap in death rates between Indigenous and non-Indigenous Australians. Alcoholic liver disease and mental and behavioural disorders were among the leading contributors of the gap due to alcohol-related death (59% and 24%, respectively) (Table D2.16.10).
Changes over time
Looking at trends in hospitalisation rates, between 2009–10 and 2018–19, the age-standardised rate for hospitalisations related to alcohol use increased by 21% for Indigenous Australians, from 723 to 915 per 100,000. There was a more rapid increase for Indigenous females (increasing by 36%, from 539 to 724 per 100,000) than Indigenous males (increasing by 11%, from 928 to 1,125 per 100,000) over the period (Table D2.16.13).
The age-standardised rate of hospitalisations related to alcohol use for non-Indigenous Australians increased by 4.5% in the decade from 2009–10 to 2018–19, while the gap in rates for Indigenous and non-Indigenous Australians increased from 483 to 665 hospitalisations per 100,000. The rate ratio ranged between 3.0 (in 2009–10) and 4.2 (in 2012–13) over the decade from 2009–10 (Table D2.16.13, Figure 2.16.6).
Figure 2.16.6: Age-standardised hospitalisation rates and changes in the gap for alcohol-related hospitalisations, by Indigenous status, Australia, 2006–07 to 2018–19
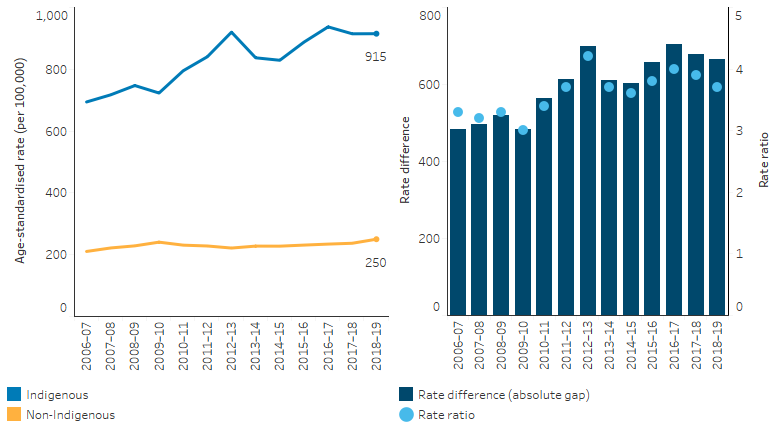
Note: Rate difference is the age-standardised rate (per 100,000) for Indigenous Australians minus the age-standardised rate (per 100,000) for non-Indigenous Australians. Rate ratio is the age-standardised rate for Indigenous Australians divided by the age-standardised rate for non-Indigenous Australians.
Source: Table D2.16.13. AIHW analysis of National Hospital Morbidity Database.
Looking at deaths due to alcohol, between 2006 and 2019 and based on age-standardised rates, the rate of alcohol-related deaths among Indigenous Australians significantly declined by 18%, and the gap between Indigenous and non-Indigenous Australians declined by 23%. However, over the decade 2010 to 2019, there was no statistically significant change in the rate of alcohol-related deaths for Indigenous or non-Indigenous Australians, nor in the gap in the rates for Indigenous and non-Indigenous Australians (Table D2.16.22, Figure 2.16.7).
Figure 2.16.7: Age-standardised mortality rates and changes in the gap due to alcohol use, by Indigenous status, NSW, Qld, WA, SA and the NT, 2006 to 2019
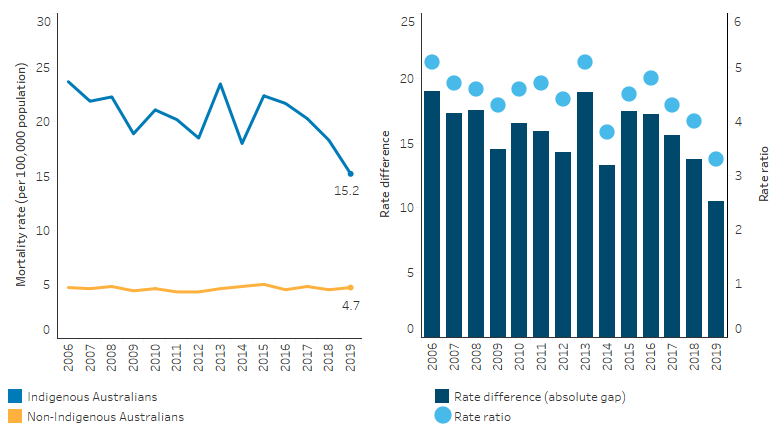
Note: Rate difference is the age-standardised rate (per 100,000) for Indigenous Australians minus the age-standardised rate (per 100,000) for non-Indigenous Australians. Rate ratio is the age-standardised rate for Indigenous Australians divided by the age-standardised rate for non-Indigenous Australians.
Source: Table D2.16.22. AIHW National Mortality Database.
Research and evaluation findings
Important differences exist between Indigenous and non-Indigenous Australians in relation to patterns and levels of consumption of alcohol, and patterns and levels of harm it can cause. Indigenous Australians are more likely to abstain from drinking alcohol than non-Indigenous Australians (30% compared with 22% in 2018–19, based on age-standardised rates). This includes lifetime abstainers and also those who used to drink but no longer do, often as a result of the harmful effects of alcohol consumption (ABS 2019; Wilson et al. 2010). However, of the Indigenous Australians who do consume alcohol, a greater proportion does so at levels that pose both short-term and long-term risks to their health and the health of others (Chikritzhs et al. 2004; Gray et al. 2018).
There is evidence to show that a range of factors contributes to the higher levels of alcohol consumption by Indigenous Australians. The social determinants contributing to the health status of Indigenous Australians include current and past inequalities, racism, intergenerational trauma and higher levels of emotional and social distress (Gray et al. 2018)
In their review of the harmful use of alcohol among Indigenous Australians, Gray et al. (2018) found the effects of alcohol on individuals are not simply a product of the substance itself. The amounts of alcohol consumed, the way in which it is consumed and the ways in which people behave under its influence are conditioned by: the characteristics of alcoholic beverages themselves and their availability, price and marketing; individual characteristics of drinkers and their life experiences and social and emotional wellbeing; and wider sociocultural settings, including the social determinants of health (Gray et al. 2018).
Drinking alcohol while pregnant may result in miscarriage, stillbirth, low birth weight, intrauterine growth restriction, preterm birth and a range of potentially lifelong physical, mental, behavioural and learning issues, collectively referred to as Fetal Alcohol Spectrum Disorders (FASD) (France et al. 2010; Mutch et al. 2015; Srikartika & O'Leary 2015). FASD encompasses neurodevelopmental disorders caused when an unborn child is exposed to alcohol in the womb. While existing research has limitations, risks of harm are said to increase with the amount and frequency of alcohol consumed (see measure 2.21 Health behaviours during pregnancy) (O'Leary et al. 2010).
Nationally, the true prevalence of FASD for Indigenous Australians is not known; estimates vary from 2.7 to 4.7 per 1,000 births (HRSCSPLA 2012). A study in the Fitzroy Valley in Western Australia found the rate to be higher, at 120 per 1,000 children (note: the small sample size of 127 pregnancies) (Fitzpatrick et al. 2015). A community-led project to lower the risk of FASD in the Fitzroy Valley has achieved outstanding results. The project was guided by Elders and the evidence-based Marulu Strategy. It was developed in consultation with research partners the Telethon Kids Institute, the University of Sydney and the George Institute for Global Health. The intervention adopted a holistic approach to lower the risk and impact of FASD through prevention, diagnosis and providing therapy support to affected individuals and families coping with lifelong physical and mental health problems. A team of 20 local Aboriginal community researchers were trained and enlisted to run the program (Fitzpatrick et al. 2017; Telethon Kids Institute 2016). Since the Marulu Strategy began in 2010, midwife-collected data revealed a dramatic fall in drinking during pregnancy in the Fitzroy Valley in response to the program, from 61.0% in 2010 to 31.9% in 2015. This was heavily influenced by the significant reduction in first-trimester alcohol use from 45.1% in 2008 to 21.6% in 2015 (Symons et al. 2020). The project also teamed up with multidisciplinary paediatric and allied health services to provide FASD diagnosis and follow-up services to the participating communities. Between 2016 and 2018, the project provided a total of 209 assessments to children, youths and adults, and supported those in need by providing a total of 458 therapy hours. The project highlighted community-led strategies (for example educating the community on the harms of alcohol consumption during pregnancy) to reduce and eliminate FASD. These provide lessons for approaches in other Indigenous and non-Indigenous communities.
Research shows a link between incarceration and FASD. A study in Western Australia—the Banksia Hill Project—was conducted in a Western Australian youth correctional facility and found that neurodevelopmental impairments due to FASD can predispose young people to engagement with the law (Bower et al. 2018). It is the first study in Australia to assess and diagnose young people in a youth custodial facility. Ninety-nine young people completed a full assessment, 93% were male and 74% were Aboriginal. Thirty-six people were diagnosed with FASD, a prevalence of 36%, the majority of which had not previously been diagnosed.
Alcohol is a major contributor to emergency department hospitalisations for injuries and interpersonal violence (Gale et al. 2015; Hides et al. 2015; Miller et al. 2012; Poynton et al. 2005). Economic literature shows that restricting access to alcohol reduces alcohol-related harm such as death, crime, and injuries (Brand et al. 2007; Carpenter & Dobkin 2009; Wagenaar et al. 2010). Evaluations of alcohol restriction interventions in the Kimberley Health Region of Western Australia provided evidence that the restriction of selling high strength alcohol has contributed to a significant reduction in alcohol-related hospitalisations and emergency department hospitalisations (Sun et al. 2019). Reducing the number of alcohol sales outlets may also be effective; the phased closure of the Aurukun tavern was most likely the cause of the 50% reduction in the number of assaults in Aurukun (DSS 2012).
The Northern Territory Government has introduced a suite of alcohol-related harm minimisation measures including the rewrite of the Northern Territory Liquor Act 1978, the October 2018 introduction of the minimum unit price (MUP) on alcohol ($1.30 per standard drink), and the roll-out of Police Auxiliary Liquor Inspectors. Several publications and evaluations have shown associations between reductions in alcohol-related harm and the introduction of these measures but it was difficult to distinguish the impact from individual interventions on outcomes.
Initial statistics released by the Northern Territory Government in September 2019 showed that since the release of the Riley Review in October 2017, the NT government’s implementation on the recommendation have led to an initial 22% reduction in alcohol-related assaults across the Northern Territory, including 40% in Alice Springs and 15.5% in Darwin, and a drop of 24.5% in alcohol-related emergency department presentations in the Northern Territory hospitals (Northern Territory Government Newsroom 2019).
A study examined the effects of the introduction of the MUP on critical care admissions in Alice Springs, Northern Territory. While more time was required to evaluate the full effect of the floor price in the context of other supply reduction measures, the study found that the proportion of patients admitted to the Alice Springs Hospital intensive care units for acute alcohol misuse had dropped by 54% in the first six months after the introduction of the policy in October 2018 (Secombe et al. 2020).
As part of an investigation into the introduction of the MUP legislation in the Northern Territory, an evaluation found a wide range of benefits to the community that have coincided with the MUP implementation. The introduction of the MUP has been associated with significant declines in: the total alcohol wholesale supply per capita; protective custody episodes, alcohol-related assaults; alcohol-related ambulance attendances and emergency department presentations; alcohol-related road traffic crashes; and child protection notifications, protection orders and out-of-home care cases. The study also showed that tourism and the number of liquor licences have not been impacted by the introduction of the MUP. However, this study only covered a limited period (Coomber et al. 2020).
A more recent evaluation of the MUP across the Northern Territory and over a longer period, found a more complex picture, although the study did not focus on Aboriginal community views or impact. The evaluation found that the MUP has been effective in reducing the supply of low-cost high-alcohol products with evidence of a decline in cask wine sales, although there was price rebalancing across other alcohol products and an increase in retail sales across a variety of other alcohol products, particularly spirits. COVID-19 also had a significant impact during the period evaluated. The evaluation found that although there had been significant reductions in alcohol-related emergency presentations in Alice Springs and Tennant Creek, this was not found in Greater Darwin. The evaluation concluded that it was difficult to attribute these emergency presentation findings to the impact of the MUP as distinct from other local policy interventions such as local licensing arrangements and the Police Auxiliary Liquor Inspectors. There was evidence of a reduction in alcohol-related non-domestic violence assaults following the suite of alcohol policy interventions made at the time of the commencement of the MUP. The evaluation recommended that the MUP be retained at the current level (Fronter economics and Yarning 2022).
Implications
Since the late 1970s, various inquiries have highlighted the link between Indigenous social disadvantage, poor health and high levels of alcohol use as a legacy of past policies (Commonwealth of Australia 1995; House of Representatives Standing Committee on Aboriginal Affairs 1977; National Aboriginal Health Strategy Working Party 1989; Royal Commission into Aboriginal Deaths in Custody 1991). While colonialism and dispossession are not the cause of all harmful alcohol use among Indigenous Australians, observed drinking patterns are a response both to this history and the current social conditions that have arisen from it, as they are among indigenous peoples elsewhere (Kirmayer et al. 2000; Saggers & Gray 1998).
The health effects of excess alcohol consumption are evident in both mortality and morbidity statistics. Alcohol is a serious public health issue facing many Indigenous Australian communities (Calabria et al. 2010). Reducing harmful alcohol and other substance misuse can significantly reduce levels of assaults and homicides and disability while improving the overall health and wellbeing of the population (SCRGSP 2009). A reduction in harmful alcohol and other substance misuse might also increase educational attainment, household and individual income levels and reduce crime and imprisonment rates (SCRGSP 2005).
A number of local, regional and national strategies, including the National Alcohol Strategy
2019–28, have been implemented over the years with the aim of reducing risky and high-risk alcohol consumption, including some that restrict supply. Some of these are whole-of-community strategies, while others are targeted solely at Indigenous Australians. At present, most legal provisions governing the supply of liquor are the responsibility of the states and territories, limiting the role the Commonwealth can directly play. In many discrete Indigenous communities in remote areas of Northern and Central Australia, alcohol is totally or partly banned. Further research and evaluations to assess the effectiveness of these strategies need to be undertaken.
The overarching principle of Australia’s National Drug Strategy is that of harm minimisation, which comprises of three pillars: demand reduction, supply reduction and harm reduction. Strategies should align with the three pillars and also address underlying social determinants, aim to prevent the uptake of harmful use, provide treatment for those who are dependent and support those whose lives are affected by others’ harmful alcohol and other drug use (Gray et al. 2018)
For those Indigenous Australians that access alcohol treatment, key themes identified for effective alcohol treatment include individual engagement, flexibility, assessment of suitability, Indigenous staff, community engagement, practical support, counselling, coping with relapse and contingency planning (Brett et al. 2014) (see measure 3.11 Access to alcohol and drug services).
Further research is warranted into what policy settings are needed to encourage interventions that will reduce the prevalence of risky and high-risk alcohol consumption and the consequent harm to health among Indigenous people and communities.
This measure uses different datasets to explore patterns of alcohol use and related health effects and harm. A potential inconsistency that needs further investigation is the survey data that may underestimate alcohol consumption. This may be particularly relevant for services in remote areas where the survey data show a lower proportion of Indigenous Australians exceeding lifetime risk guidelines compared with non-remote areas, while hospitalisation rates of alcohol-related conditions in remote areas and the Northern Territory are much higher than other areas. This could point to issues around the availability of services in remote areas and also potentially higher quantities of alcohol consumed beyond the four-drink data category captured in the 2018–19 National Aboriginal and Torres Strait Islander Health Survey data. To illustrate, the 2012–13 Australian Aboriginal and Torres Strait Islander Health Survey captured 24-hour recall of amounts of alcoholic beverages consumed by Indigenous adults. This found that the median amount of alcoholic beverages consumed by Indigenous adults was higher in remote areas (1,717 grams) than non-remote areas (1,007 grams).
Aboriginal Community Controlled Health Services (ACCHSs) have made important contributions to improving the health of Indigenous Australians through the provision of culturally appropriate health care. ACCHSs vary in size, and the services they offer reflect the unique health needs of an individual community. Advocacy efforts of ACCHSs have been shown to improve alcohol-related policies that are associated with a reduction in alcohol-related assaults and alcohol-related presentations to health services (Campbell et al. 2018). ACCHSs can play a pivotal role in providing specific and culturally relevant alcohol services and should be considered in the development of alcohol harm prevention or reduction strategies.
The Health Plan is the overarching policy framework to drive progress against the Closing the Gap health targets and priority reforms. Implementation of the Health Plan aims to drive structural reform towards models of care that are prevention and early intervention focused, with greater integration of care systems and pathways across primary, secondary and tertiary care. It also emphasises the need for mainstream services to address racism and provide culturally safe and responsive care, and be accountable to Aboriginal and Torres Strait Islander people and communities.
Priority 4 of the Health Plan focuses on health promotion and emphasises the role of cultural and social determinants of health. It seeks to harness the protective aspects of culture, with place-based evidence informed action. Health promotion seeks to empower people to make decisions that prevent ill health before it occurs, including through access to information, and opportunities for making healthy choices.
Priority 4 includes Objective 4.6: Deliver targeted, needs-based and community-driven actions to prevent alcohol and other drug related harm. Prevention effort must be trauma-aware and healing-informed. The Health Plan recognises the importance of delivering prevention and treatment activities in genuine partnership or even led by local communities, preferably through ACCHSs.
References
- ABS (Australian Bureau of Statistics) 2013. Australian Aboriginal and Torres Strait Islander Health Survey: First Results Australia 2012–13. cat. no. 4727.0.55.001. Canberra: AIHW.
- ABS 2019. National Aboriginal and Torres Strait Islander Health Survey, 2018–19. 4715.0. Canberra: ABS.
- AIHW (Australian Institute of Health and Welfare) 2022. Australian Burden of Disease Study: Impact and causes of illness and death in Aboriginal and Torres Strait Islander people 2018. Canberra: AIHW
- Bower C, Watkins RE, Mutch RC, Marriott R, Freeman J, Kippin NR et al. 2018. Fetal alcohol spectrum disorder and youth justice: a prevalence study among young people sentenced to detention in Western Australia. BMJ Open 8.
- Brand DA, Saisana M, Rynn LA, Pennoni F & Lowenfels AB 2007. Comparative analysis of alcohol control policies in 30 countries. PLoS medicine 4:e151.
- Brett J, Lawrence L, Ivers R & Conigrave K 2014. Outpatient alcohol withdrawal management for Aboriginal and Torres Strait Islander Australians. Australian Family Physician 43:563-6.
- Calabria B, Doran CM, Vos T, Shakeshaft AP & Hall W 2010. Epidemiology of alcohol‐related burden of disease among Indigenous Australians. Australian and New Zealand journal of public health 34:S47-S51.
- Campbell MA, Hunt J, Scrimgeour DJ, Davey M & Jones V 2018. Contribution of Aboriginal Community-Controlled Health Services to improving Aboriginal health: an evidence review. Australian Health Review 42:218-26.
- Carpenter C & Dobkin C 2009. The effect of alcohol consumption on mortality: regression discontinuity evidence from the minimum drinking age. American Economic Journal: Applied Economics 1:164-82.
- Chikritzhs T, Gray D, Stockwell T, Stearne A, Pascal R & Saggers S 2004. Applying national indicators of alcohol-related harms to Indigenous Australians: a discussion paper. National Drug Research Institute, Curtin University of Technology, Perth.
- Commonwealth of Australia 1995. Alcohol report, race discrimination, human rights and the distribution of alcohol. Canberra: Race Discrimination Commissioner.
- Coomber K, Miller P, Taylor N, Livingston M, Smith J, Buykx P et al. 2020. Investigating the introduction of the alcohol minimum unit price in the Northern Territory (FINAL REPORT). Deakin University, Geelong Australia.: Prepared for the Northern Territory Department of Health.
- DSS (Department of Social Services) 2012. Cape York Welfare Reform Evaluation. Canberra: DSS.
- Fitzpatrick JP, Latimer J, Carter M, Oscar J, Ferreira ML, Carmichael Olson H et al. 2015. Prevalence of fetal alcohol syndrome in a population-based sample of children living in remote Australia: the Lililwan Project. Journal of paediatrics and child health 51:450-7.
- Fitzpatrick JP, Oscar J, Carter M, Elliott EJ, Latimer J, Wright E et al. 2017. The Marulu Strategy 2008–2012: overcoming fetal alcohol spectrum disorder (FASD) in the Fitzroy Valley. Australian and New Zealand journal of public health 41:467-73.
- France K, Henley N, Payne J, D'Antoine H, Bartu A, O'Leary C et al. 2010. Health professionals addressing alcohol use with pregnant women in Western Australia: barriers and strategies for communication. Substance Use & Misuse 45:1474-90.
-
Fronter economics and Yarning 2022. Evaluation of Minimum Unit Price of Alcohol in the Northern Territory. Prepared for the Northern Territory Department of Health.
- Gale M, Muscatello DJ, Dinh M, Byrnes J, Shakeshaft A, Hayen A et al. 2015. Alcopops, taxation and harm: a segmented time series analysis of emergency department presentations. BMC Public Health 15:468.
- Gray D, Cartwright K, Stearne A, Saggers S, Wilkes E & Wilson M 2018. Review of the harmful use of alcohol among Aboriginal and Torres Strait Islander people. Australian Indigenous HealthInfoNet.
- Hides L, Limbong J, Vallmuur K, Barker R, Daglish M & Young RM 2015. Alcohol‐related emergency department injury presentations in Queensland adolescents and young adults over a 13‐year period. Drug and alcohol review 34:177-84.
- House of Representatives Standing Committee on Aboriginal Affairs 1977. Alcohol problems of Aboriginals: final report. . Canberra: House of Representatives Standing Committee on Aboriginal Affairs.
- House of Representatives Standing Committee on Indigenous Affairs 2015. Alcohol, hurting people and harming communities: Inquiry in to the harmful use of alcohol in Aboriginal and Torres Strait islander communities. Canberra.
- HRSCSPLA (House of Representatives Standing Committee on Social Policy and Legal Affairs) 2012. FASD: The Hidden Harm - Inquiry into the prevention, diagnosis and management of Fetal Alcohol Spectrum Disorders. Canberra: The Parliament of the Commonwealth of Australia.
-
Kirmayer LJ, Brass GM & Tait CL 2000. The Mental Health of Aboriginal Peoples: Transformations of Identity and Community. The Canadian Journal of Psychiatry 45:607-16.
- Miller P, Coomber K, Sønderlund A & McKenzie S 2012. The long‐term effect of lockouts on alcohol‐related emergency department attendances within Ballarat, Australia. Drug and alcohol review 31:370-6.
- Mutch RC, Watkins R & Bower C 2015. Fetal alcohol spectrum disorders: notifications to the Western Australian Register of Developmental Anomalies. Journal of Paediatrics & Child Health 51:433-6.
- NHMRC (National Health and Medical Research Council) 2008. Australian alcohol guidelines for low-risk drinking 2007.
- NHMRC 2020. Australian Guidelines To Reduce Health Risks From Drinking Alcohol. (ed., Department of Health). Department of Health: National Health and Medical Research Council.
- Northern Territory Government Newsroom 2019. Blood Alcohol Limit on Vessels Deferred: Alcohol Harm Minimisation Plan Update Released.
- O'Leary CM, Nassar N, Kurinczuk JJ, de Klerk N, Geelhoed E, Elliott EJ et al. 2010. Prenatal Alcohol Exposure and Risk of Birth Defects. Pediatrics.
- Poynton S, Donnelly N, Weatherburn D, Fulde G & Scott L 2005. Role of Alcohol in Injuries Presenting to St Vincent’s Hospital Emergency Department and the Associated Short-term Costs, The. BOCSAR NSW Alcohol Studies Bulletins:16.
-
Royal Commission into Aboriginal Deaths in Custody 1991. Royal Commission into Aboriginal Deaths in Custody: National reports [Vol 1-5], and regional reports. Canberra: Australian Government Publishing Service.
-
Saggers S & Gray D 1998. Dealing with alcohol : indigenous usage in Australia, New Zealand and Canada. Melbourne: Cambridge University Press.
- SCRGSP (Steering Committee for the Review of Government Services Provision) 2005. Overcoming Indigenous disadvantage: key indicators 2005. Canberra: Productivity Commission.
- SCRGSP 2009. Overcoming Indigenous disadvantage: key indicators 2009. Canberra: Productivity Commission.
- Secombe PJ, Stewart P, Brown A, Bailey MJ & Pilcher D 2020. The impact of an alcohol floor price on critical care admissions in Central Australia. The Medical Journal of Australia 5:212.
- Srikartika VM & O'Leary CM 2015. Pregnancy outcomes of mothers with an alcohol-related diagnosis: a population-based cohort study for the period 1983-2007. BJOG: An International Journal of Obstetrics & Gynaecology 122:795-804.
- Stevenson RJ, Lind B & Weatherburn D 1999. Property damage and public disorder: their relationship with sales of alcohol in New South Wales, Australia. Drug & Alcohol Dependence 54:163-70.
- Stockwell T, Donath S, Cooper-Stanbury M, Chikritzhs T, Catalano P & Mateo C 2004. Under-reporting of alcohol consumption in household surveys: a comparison of quantity-frequency, graduated-frequency and recent recall. Addiction 99:1024-33.
- Sun W, Jian L, Xiao J, Akesson G & Somerford P 2019. The impact of alcohol restriction on hospital and emergency department service utilizations in two remote towns in the Kimberley Region of Western Australia. Frontiers in Public Health 7:17.
-
Symons M, Carter M, Oscar J, Pearson G, Bruce K, Newett K et al. 2020. A reduction in reported alcohol use in pregnancy in Australian Aboriginal communities: a prevention campaign showing promise. Australian and New Zealand journal of public health 44:284-90.
- Telethon Institute for Child Health Research 2009. Alcohol and pregnancy and fetal alcohol spectrum disorder: a resource for health professionals (1st revision). Perth: Telethon Institute.
- Telethon Kids Institute 2016. Making FASD History in the Fitzroy Valley. Perth, WA: : Telethon Kids Institute.
- Wagenaar AC, Tobler AL & Komro KA 2010. Effects of alcohol tax and price policies on morbidity and mortality: a systematic review. American journal of public health 100:2270-8.
- Wilson M, Stearne A, Gray D & Saggers S 2010. The harmful use of alcohol amongst Indigenous Australians. Australian Indigenous HealthInfoNet.
Related measures
- 1.03 Injury and poisoning
- 1.04 Respiratory disease
- 1.05 Cardiovascular disease
- 1.07 High blood pressure
- 1.18 Social and emotional wellbeing
- 2.10 Community safety
- 2.11 Contact with the criminal justice system
- 2.21 Health behaviours during pregnancy
- 3.03 Health promotion
- 3.11 Access to alcohol and drug services